Screening
The goal of a screening and surveillance program for BE is to identify individuals at risk for progression to esophageal adenocarcinoma
- Screening for BE may be considered in men with chronic (>5 years) and/or frequent (weekly or more) symptoms of gastroesophageal reflux (heartburn or acid regurgitation) and two or more risk factors for BE or Esophageal Adenocarcinoma (EAC). These risk factors include: age >50 years, Caucasian race, presence of central obesity, current or past history of smoking, and a confirmed family history of BE or EAC (in a first-degree relative)
- Given the substantially lower risk of EAC in females with chronic GER symptoms (when compared with males), screening for BE in females is not recommended. However, screening could be considered in individual cases as determined by the presence of multiple risk factors for BE or EAC (age >50 years, Caucasian race, chronic and/or frequent GERD, central obesity, current or past history of smoking, and a confirmed family history of BE or EAC (in a first-degree relative))
- Screening of the general population is not recommended
The good news about Barrett’s Esophagus is that it can be treated. The options for management and eradication of Barrett’s have evolved over the years, and physician practice habits are changing as more options become available. Surveillance and medical management have been the pre-dominant management strategies for Barrett’s for years. But these strategies were only applicable to the earliest forms of Barrett’s and were focused more on catching the progression to worsening grades. The morbidity associated with surgery encouraged the development of endoscopic techniques for Barrett’s removal, both through resection and ablation. In recent years, new endoscopic therapies have emerged that are successfully treating the disease before it progresses to cancer. As these technologies have proven themselves effective and safe, their use in the management of Barrett’s has grown significantly over the past several years
Surveillance
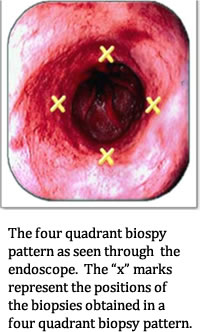
In the practice of surveillance, the physician performs an endoscopy and takes samples of the suspected Barrett’s tissue. Physicians are encouraged to use the “Seattle Protocol”, which requires biopsy samples every 1 cm to 2 cm in 4 quadrants. So if there was a 4 cm section of Barrett’s, that would be up to 16 biopsies.
According to the ACG guidelines (2018), in patients with suspected BE, at least 8 random biopsies should be obtained to maximize the yield of IM on histology.In patients with short (1–2 cm) segments of suspected BE in whom 8 biopsies are unattainable, at least 4 biopsies per cm of circumferential BE, and one biopsy per cm in tongues of BE, should be taken.
In patients with suspected BE and lack of IM on histology, a repeat endoscopy should be considered in 1–2 years of time to rule out BE.
The length of time between surveillance procedures varies and is largely up to the physician. The ACG (2018) recommends the following surveillance protocol:
- For BE patients without dysplasia, endoscopic surveillance should take place at intervals of 3 to 5 years
- Patients diagnosed with BE on initial examination do not require a repeat endoscopy in 1 year for dysplasia surveillance
- For patients with indefinite for dysplasia, a repeat endoscopy after optimization of acid suppressive medications for 3–6 months should be performed. If the indefinite for dysplasia reading is confirmed on this examination, a surveillance interval of 12 months is recommended
- For patients with confirmed low-grade dysplasia and without life-limiting comorbidity, endoscopic therapy is considered as the preferred treatment modality, although endoscopic surveillance every 12 months is an acceptable alternative
- Patients with BE and confirmed high-grade dysplasia should be managed with endoscopic therapy unless they have life-limiting comorbidity
There are some limitations to a managing Barrett’s with surveillance. Patient compliance is a major factor in surveillance intervals: When something doesn’t hurt or bother you, it’s easy to “forget” your next endoscopy. The technique only monitors the Barrett’s, looking for progression to a more severe grade. This has been called out as a contributing factor to patient anxiety. Imagine having a pre-cancerous lesion managed by a biopsy every 3-5 years.
Biopsy
According the ACG (2018), endoscopic surveillance has numerous shortcomings. Dysplasia may not be visible endoscopically and the distribution of dysplasia and cancer is highly variable. Even the most thorough biopsy surveillance programs have the potential for sampling error. Current surveillance programs are expensive and time consuming
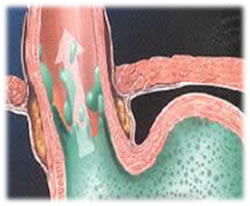
In some cases, endoscopically normal appearing squamous tissue may grow on top of Barrett's lining. When this occurs, the Barrett's lining is not only still there, but looks like normal squamous lining through the endoscope. This can lead one to think that the Barrett's is gone when it is simply buried beneath normal appearing squamous lining. This is often referred to as SSIM (subsquamous intestinal metaplasia) or buried glands.
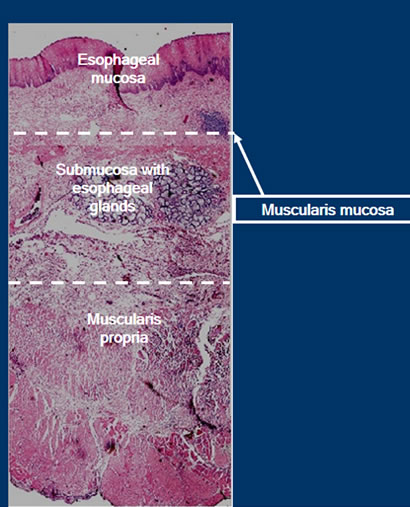
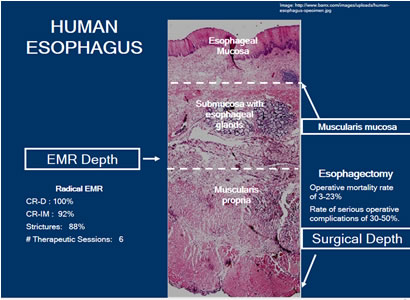
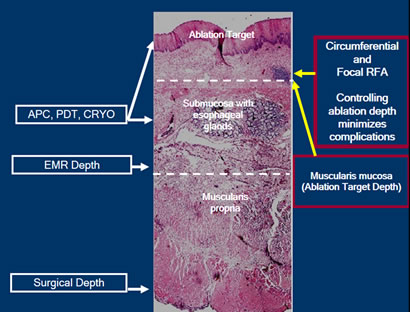
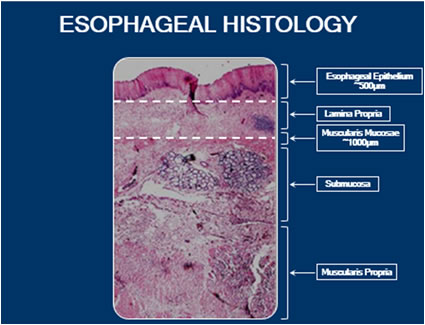
A biopsy of the human esophagus takes place at the depth of the lamina propria/muscularis mucosa layer, as illustrated in the preceding figure. The depth is adequate for tissue acquisition to send to pathology, but there are some issues to consider. Biopsies are inconsistent in terms of where they are obtained along the esophagus.
Sampling error refers to a situation where pathology exists but is missed because the clinician did not choose that area to sample. You can endoscopically see Intestinal Metaplasia (IM), but there may be an advanced grade of Barrett’s in an area that was not sampled. There is a risk that surveillance biopsy may have missed tissue with a more severe diagnosis.
Enhanced Imaging
Enhanced imaging may provide better detection. Techniques such as narrow band imaging (NBI) and chromoendoscopy show promise for better detection of dysplasia in Barrett’s esophagus. In fact, clinicians have reported numerous advantages using these new, advanced techniques:
- Changes in mucosal and vascular patterns can be identified which can predict histology indicative of dysplasia, resulting in a potentially improved ability to screen for Barret's Esophagus, detect dysplasia in established Barrett’s Esophagus and detect recurrent dysplasia/neoplasia after ablation.
- Abnormal mucosal/vascular patterns reliably mark advanced dysplasia and early esophageal adenocarcinoma.
- When used with targeted biopsy, these techniques may reduce dependency on random biopsies.
- Fewer biopsies per patient and higher proportion of dysplasia identified, compared to standard white light endoscopy.
Diagnostic yield for dysplasia or cancer increased by 34% when NBI added, when compared to White Light Endoscopy with random biopsies.
Narrow band imaging (NBI) is a high-resolution endoscopic technique that enhances the fine structure of the mucosal surface without the use of dyes.
Chromoendoscopy involves the topical application of stains or pigments to improve tissue localization, characterization, or diagnosis during endoscopy. The stains used for chromoendoscopy are transient, unlike the stains used to tattoo lesions, and the equipment needed for chromoendoscopy is widely available. These imaging techniques are simple, quick, inexpensive and safe.
Surgery-Esophagectomy
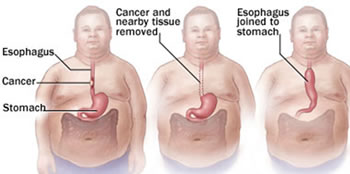
There are instances where the complete resection of Barrett’s is necessary. Esophagectomy has been an option that has been reserved for patients with high-grade dysplasia and cancer. Surgical depth is down to the Muscularis Propria. In the hands of an experienced esophageal surgeon who performs these surgeries in a center experienced in the care of patients undergoing esophagectomy, the mortality rate is around 1-8%. On the other hand, the surgical mortality in low volume centers is in the range of 16-23%.
The rate of serious complication ranges from 30-50% post esophagectomy, resulting in a poor quality of life for the patients. These can include post-operative complications such as esophageal anastomotic leak, pneumonia, deep vein thrombosis, gastric necrosis, cardiac arrhythmias, wound infections, prolonged ileus (lack of bowel function), GI bleeding, stenosis and diarrhea.
Endoscopic Mucosal Resection (EMR)
Endoscopic Mucosal Resection, or EMR, is the process of endoscopic resection of Barrett’s lesions. EMR is often used for raised lesions or advanced disease. These are often referred to as “nodules”. Physicians may choose EMR if they suspect there is already a cancer in a suspicious area, or if they would like a larger area for histological samples. It is an excellent alternative to esophagectomy when you have nodularity or small focal areas of advanced disease because it preserves the esophagus. EMR can be done as a primary treatment for the focal lesion. It can be complemented by other therapies for the larger, flat areas of disease.
There are several techniques used for EMR; the two common techniques will be explored here.
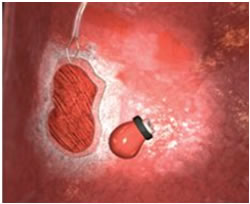
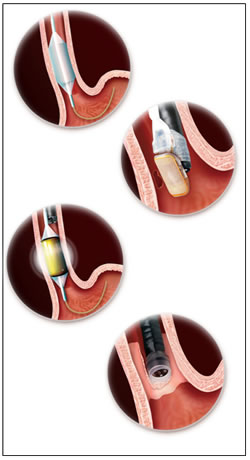
Technique One: This is done by using a small cap with a small wire loop that fits on the end of the endoscope. The nodule is suctioned into the cap and the wire loop is closed while cautery is applied.

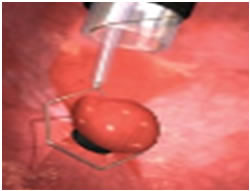
Step 1: Injection of target lesion.
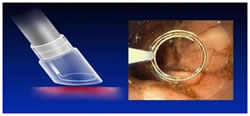
Step 2: Positioning the snare.
Step 3: Suction & snare of lesion.
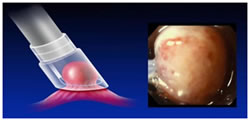
Technique Two: This is done by using a small ligation band, followed by a cautery loop. The cautery loop is around the nodule and energy is applied. Once the nodule is released from the mucosal wall, it is retrieved in the usual fashion.
EMR is very successful in removing large areas of tissue. It enables evaluation of changes in diseased tissue and can be used to obtain large biopsies for diagnosis and local tumor staging. Frequently, EMR reveals more advanced tumor stages. It is often recommended in combination with additional ablation techniques.
EMR does have some limitations. Because the resecting is down to the level of the submucosa, there is a risk for strictures. When injury is caused to the submucosa, there is a risk of stricture formation. This can limit its utilization to advanced disease, so often focal EMR is complemented with an ablation technique in a broad field of flat disease.
EMR/Mucosectomy target depth is into the submucosa. This preserves the esophagus, while removing a substantial piece of tissue. One technique is to remove all of the Barrett’s tissue through a Stepwise Radical Endoscopic Resection (SRER). SRER is a technique in which the complete Barrett’s Esophagus segment is removed in consecutive endoscopic resection sessions. Retrieval of the entire Barrett’s Esophagus segment for histological assessment is ideal, as it may permit referral to surgery for advanced lesions. Single-center studies have shown excellent results of SRER for HGD or early cancer. An important limitation of SRER is the rate of complications, such as esophageal stenosis requiring dilation. Focal EMR is when there is only a resection of certain areas. EMR is successful at removing these focal areas, but there still is the risk of scarring and the potential for strictures.
Argon Plasma Coagulation (APC)
Argon-plasma coagulation (APC) is a widely used, contact-free, operator dependent endoscopic ablation technique for the eradication of BE with the relevant risk of stricture formation and buried metaplastic glands under a layer of neosquamous epithelium. Hybrid APC, which combines APC with submucosal saline injection, was developed to address these complications. The Barrett epithelium is lifted with a 0.9% saline injection using a high-pressure water jet, creating a safety cushion under the mucosa. The Barrett esophagus can then be ablated more thoroughly and with a higher energy setting, without an increase in side effects or complications.
In a pilot study of 50 patients conducted by H. Manner et.al (2015), Hybrid-APC was found effective and safe for BE ablation in a tertiary referral center. The rate of stricture formation was only 2%, compared with a 5-10% stricture formation after thermal ablation. Further studies are required to confirm the present results.
There is a certain user variability as it related to the duration of the application and how close to place the tip to the mucosa in order to be effective. This affects the depth of the burn, and recall that Barrett’s lives in the ½ millimeter range. The optimum ablation depth is 1mm. Focal APC does not have a mechanism to control the depth of burn, so the depth can be variable based on the user application. This includes how close the catheter is placed to the tissue and how long the energy is applied.
Photodynamic Therapy (PDT)
PDT, or Photodynamic Therapy, is a treatment that is used as an alternative to surgery in non-surgical candidates for the treatment of high-grade dysplasia and early cancers. It was the first medical technology that demonstrated a decrease in progression rates to cancer in HGD patients. It can also be used to reduce the tumor mass in patients with advanced esophageal cancer.
PDT Technique:
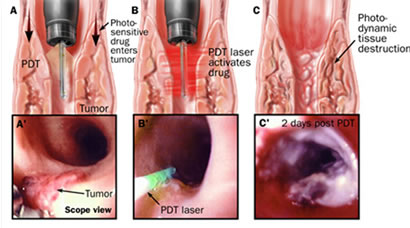
- PDT uses a combination of photosensitizer--a light-activated drug-- and laser light to destroy abnormal cells. PDT patients are injected with a photosensitizer to render their tissue extremely sensitive to laser light.
- The lesion is then illuminated with a laser light of proper power and wavelength, or color.
- The interaction of laser light and the photosensitizer causes a chemical reaction, killing the abnormal cells.
PDT tends to affect the esophagus to the submucosal layer. While effective, it can produce some complications. Results vary in the 51-77% response rate. In studies the application was not circumferential, and in some instances, exceeded well into the submucosal tissue, and in others, not deep enough into the epithelium.
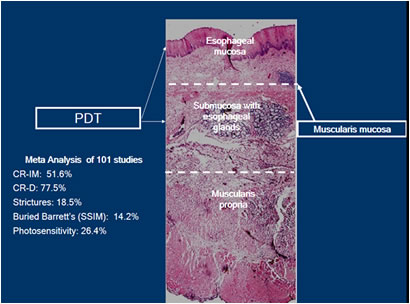
Although PDT was the first therapy to show significant decrease in high grade dysplasia and cancer in patients with BE, its use has been limited, primarily because of its costs and its complications:
- Photosensitivity (can persist from 30-90 days after injection with the photosynthesizing drug)
- Strictures (tend to occur in about one third of patients treated, and normally happen 3 to 4 weeks after therapy)
- Subsquamous Barrett’s mucosa (buried Barrett’s can be found when the Barrett’s mucosa is not eliminated by therapy and is overgrown by surrounding squamous mucosa)
- Chest pain
- Nausea
- Vomiting
Cryotherapy
By freezing tissues to extreme cold temperatures, cryotherapy attempts to remove abnormal cells and allow for the re-growth of new, healthy cells in their place. Cryotherapy has been used in patients with Barrett’s esophagus with high-grade dysplasia and persistent low-grade dysplasia as well as early stage esophageal cancer that is not amenable to standard therapies, including surgery, chemotherapy and radiation therapy. There are two different cryogens. One is a rapid flow CO2 stored at room temperature as a cryogen source and a catheter to deliver the cryogen to the treatment site. By utilizing the Joule-Thompson effect, the CO2 expands and rapidly cools to -78C as it exits the catheter. Another is a system that transports low-pressure liquid nitrogen through a specially designed catheter that is passed through a standard endoscope. This freezes the desired tissue. It utilizes large volumes of gas, which requires a second catheter to be placed so it can continuously remove the gas.
It is reported that three to eight treatments are necessary in order to see any measurable results. There is a lack of substantial data that enables researchers to conclude if depth of ablation is sufficient, but the current data suggests that it’s around 1mm to 2mm in depth. Because Cryotherapy is also uncontrolled and user-dependent those depths can vary significantly.
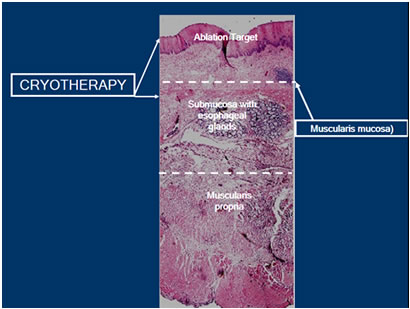
As an effective treatment modality, cryotherapy has distinct advantages and disadvantages. One advantage is that it is through the scope. One important limitation to cryotherapy is that there is no visual endpoint that lets you know when enough treatment has been performed. So it’s up to the user to decide when to stop the application of the therapy. This would account for uncontrolled depth of ablation.
Radiofrequency Ablation
 Radiofrequency Ablation is commonly referred to as RFA. RFA is indicated for ablation of Barrett’s esophagus, which may include non-nodular, ND-IM, LGD and HGD.
Radiofrequency Ablation is commonly referred to as RFA. RFA is indicated for ablation of Barrett’s esophagus, which may include non-nodular, ND-IM, LGD and HGD.
RFA has a few key treatment goals, one of which is the delivery of ablative energy in less than one second, allowing long or short segments of BE to be treated quickly. It provides a consistent application of bipolar energy that uniformly removes the esophageal epithelium. It is a contact probe, in contrast to other therapies that are non-contact. RFA can be done circumferentially with a balloon based system for long segment BE or a more focal device ffor short segment or islands of BE. .
RFA’s controlled treatment depth of less than 1 millimeter (or to the Muscularis Mucosae) reduces the risk of stricture formation. This also reduces the potential for buried glands and improves patient tolerability.
After Barrett’s is confirmed by a pathologist based on a prior EGD, the patient is scheduled for ablation.
During the ablation procedure, the distal and proximal margins of the disease are noted
For long segment Barrett’s (3cm), the physician introduces an ablation balloon over a guide wire and positions it in the area to be ablated. A special generator then delivers the energy to the balloon. This area is cleaned, and the ablation steps are repeated. It is a process designed to insure a uniform ablation depth and to minimize complications.
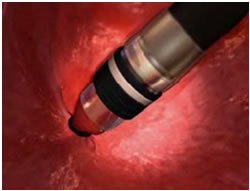
To treat short segment or islands of Barrett’s, a focal catheter is mounted on the tip of the scope to deliver the energy. Each area is ablated twice.
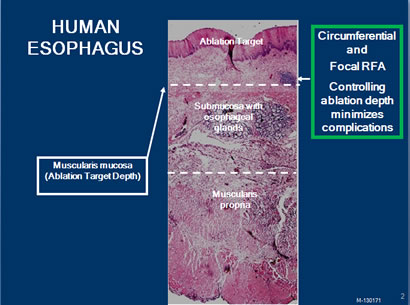
As you review the following graphic, note that the ablation is to the muscularis mucosa. This is deep enough to eliminate the columnar epithelium and underlying lamina propria. Typically, buried glands will be present in these layers, so they are ablated simultaneously. When the Barrett’s tissue is eliminated, normal squamous epithelium grows back in its place.
There is a significant amount of research that has gone into the study of RFA to ensure that it consistently works and remains safe:
Long term data
- RFA resulted in complete eradication of disease in 98% of NDBE patients, with 2.5-years follow-up.
- At 5 years, 92% of patients maintained durable cure, and no patients demonstrated neoplastic progression.
Rigorous Randomized control trial for Dysplasia published in the New England Journal of Medicine
- Complete Response Barrett’s: 83%
- Complete response Low Grade Dysplasia: 95%
- Complete response High Dysplasia: 90%
Compared to a diagnostic EGD, an RFA procedure is therapeutic, therefore takes longer. Multiple intubations extend the procedure time and can affect the patient with a sore throat lasting a day or so. Possible complications may include mucosal laceration, acute bleeding and esophageal stricture. The delivery of the energy is automated, so it eliminates the user variability and the duration of the application of therapy. This controls the depth of ablation, insuring effectiveness while limiting complications. With 68+ publications to date, it is the most well-research Barrett’s ablation device available today. The studies consistently show a 90+% efficacy rate, which means complete elimination of all Barrett’s tissue.
Goals of Treatment
- Eliminating the entire at risk mucosa
- Minimizing complications
- Minimizing recurrence, strictures and bleeding
- Decreasing the need for frequent surveillance
To meet these objectives, the correct depth ablation should target to, but not beyond, the muscularis mucosa. This is desired to eliminate all intestinal metaplasia, but also to avoid complications.
Focal APC is uncontrolled, and no studies have documented a consistent depth of burn. PDT application is effective, but associated complications and inconsistent efficacy limit its widespread utilization. Cryotherapy data is not substantial to date to recognize if depth of ablation is sufficient. However, data suggest that it’s around 1-2 mm in depth. EMR has a role when early cancers or Barrett’s tissue extends into the submucosa. Stricturing tends to limit its utilization to Barrett’s nodules.


 The grading of Barrett’s Esophagus can be analogous to a person wading out into the ocean:
The grading of Barrett’s Esophagus can be analogous to a person wading out into the ocean:


